Fierce Pharma
Fierce Biotech
Fierce Healthcare
Fierce Life Sciences Events
Advertise
About Us
Providers
Hospitals
Practices
Retail
Health Tech
AI and Machine Learning
Digital Health
Telehealth
Payers
Regulatory
Finance
Special Reports
Fierce 50
Special Report
Awards Gala
Resources
Webinars
Fierce Events
Industry Events
Podcasts
Survey
Whitepapers
Events
Subscribe
Subscribe
Providers
Hospitals
Practices
Retail
Health Tech
AI and Machine Learning
Digital Health
Telehealth
Payers
Regulatory
Finance
Special Reports
Fierce 50
Special Report
Awards Gala
Resources
Webinars
Fierce Events
Industry Events
Podcasts
Survey
Whitepapers
Events
Subscribe
Fierce Pharma
Fierce Biotech
Fierce Healthcare
Fierce Life Sciences Events
Advertise
About Us
Hospitals
Providers
Acute, behavioral revenue gains push UHS to $262M Q1 profit
The company topped estimates as same-store per-patient revenue metrics jumped on both sides of its business.
Dave Muoio
Apr 24, 2024 11:39pm
CHS logs expected Q1 net loss but beats on revenues
Apr 24, 2024 10:38pm
UPMC laying off roughly 1,000 workers
Apr 24, 2024 3:00pm
CHA sues Anthem Blue Cross over discharge delays
Apr 24, 2024 1:34pm
Gold seal of approval comes to telehealth market
Apr 24, 2024 9:05am
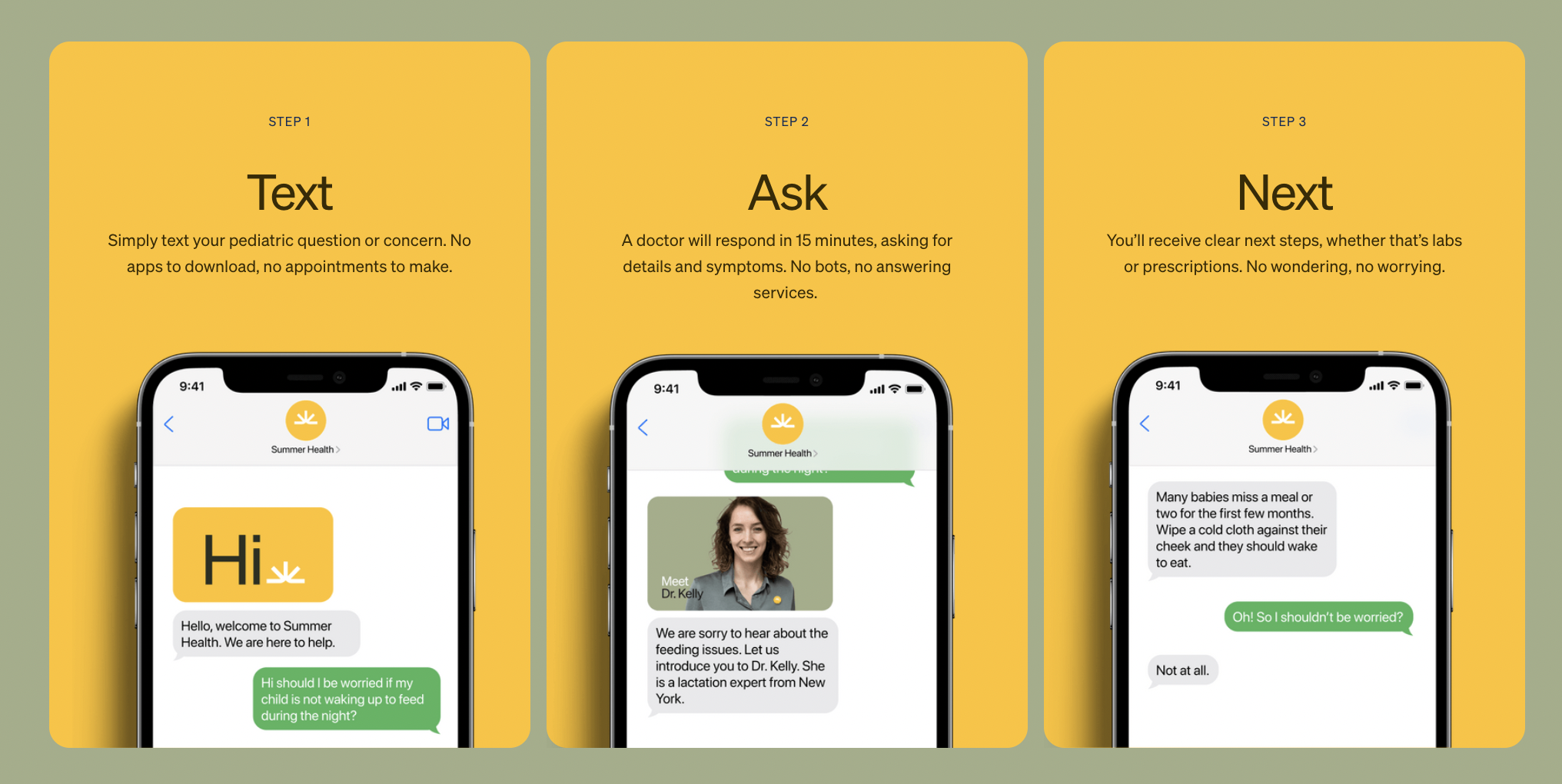
Summer Health pockets $12M for text-based pediatric service
Apr 24, 2024 8:00am